|
|
||||||||
|
|
| Home |
Volume 8: No. 6, November 2011
Suggested citation for this article: Hoerger TJ, Wittenborn JS, Young W. A cost-benefit analysis of lipid standardization in the United States. Prev Chronic Dis 2011;8(6):A136 http://www.cdc.gov/pcd/issues/2011/nov/10_0253.htm. Accessed [date].
PEER REVIEWED
Introduction
By improving lipid standardization, the Centers for Disease Control and Prevention’s (CDC’s) Lipid Standardization Program and Cholesterol Reference
Method Laboratory Network have contributed to the marked reduction in heart
disease deaths since 1980. The objective of this study was to estimate the
benefits (ie, the value of reductions in heart disease deaths) and costs
attributable to these lipid standardization programs.
Methods
We developed a logic model that shows how the inputs and activities of the lipid standardization programs produce short- and medium-term outcomes that in turn lead to improvements in rates of cardiovascular disease and death. To calculate improvements in long-term outcomes, we applied previous estimates of the change in heart disease deaths between 1980 and 2000 that was attributable to statin treatment and to the reduction in total cholesterol during the period. Experts estimated the share
of cholesterol reduction that could be attributed to lipid standardization. We applied alternative assumptions about the value of a life-year saved to estimate the value of life-years saved attributable to the programs.
Results
Assuming that 5% of the cholesterol-related benefits were attributable to the programs and a $113,000 value per life-year, the annual benefit attributable to the programs was $7.6 billion. With more conservative assumptions (0.5% of cholesterol-related benefits attributable to the programs and a $50,000 value per life-year), the benefit attributable to the programs was
$338 million. In 2007, the CDC lipid standardization programs cost $1.7 million.
Conclusion
Our estimates suggest that the benefits of CDC’s lipid standardization programs greatly exceed their costs.
Cholesterol awareness and control are important factors in reducing deaths from heart disease in the United States and are a key focus of health promotion and clinical practice (1). Age-adjusted death rates for heart disease have dropped in the United States from 1980 (412.1 per 100,000 population) to 2000 (257.6 per 100,000 population) and 2006 (200.2 per 100,000 population) (2,3). Using a model of the impact of various risk factors and treatments on heart disease deaths, Ford et al (4) and Capewell et al (5) attributed nearly one-third of the reduction in heart disease deaths between 1980 and 2000 to a reduction in the prevalence of high cholesterol and improved secondary prevention using statin drugs to control cholesterol in people with previous heart disease.
An important but sometimes overlooked contribution to improvements in cholesterol awareness and control has been provided by the Centers for Disease Control and Prevention’s (CDC’s) Lipid Standardization Program (LSP) and Cholesterol Reference Method Laboratory Network (CRMLN) (“lipid standardization programs” hereafter). The LSP is an accuracy-based program that defines benchmark reference methods and maintains stable pools of reference testing materials (6,7). Its standardization activities have supported epidemiologic studies that identified the role of cholesterol in heart disease and clinical research laboratories that conducted standardized clinical trials to test the effects of alternative treatments to reduce cholesterol. The CRMLN is a network of laboratories replicating the CDC reference methods to help manufacturers improve the accuracy of clinical testing methods (8). Because only a few manufacturers produce the diagnostic equipment and supplies used in cholesterol testing, facilitating accurate manufacturer calibration results in more accurate clinical testing nationwide (9).
As a cost-saving measure, in 2008 the National Heart, Lung, and Blood Institute (NHLBI) retracted its 50-year budgetary commitment to the LSP. Without the NHLBI funding, the LSP and CRMLN programs may not be able to continue in their present form. In response, the Cardiovascular Biomarker Standardization Steering Committee of the National Association of Chronic Disease Directors (NACDD) asked NACDD to conduct a cost-benefit study of the LSP. The objective of this study was to estimate the benefits and costs of the LSP and CRMLN. Results of the study may be used by policy makers to determine the value of lipid standardization.
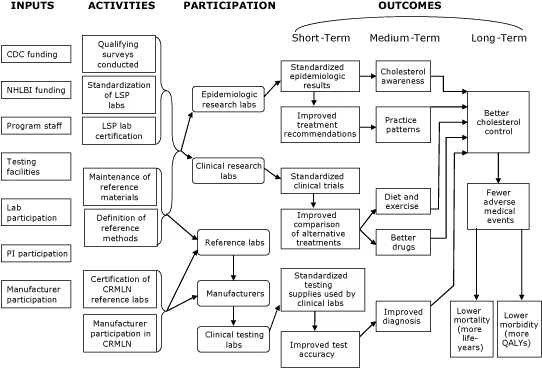
We first developed a logic model for assessing the impact of the CDC lipid standardization programs (Figure 1). Logic models are a program evaluation tool used to graphically depict major elements and causality pathways of a program (10). The left side of the logic model lists the resources (inputs) necessary for program operation. The logic model then shows the major program activities; the participants involved with and affected by these activities; and the short-, medium-, and long-term outcomes of the programs.
Figure 1. Lipid Standardization Program (LSP) and Cholesterol Reference Method Laboratory Network (CRMLN) logic model. Abbreviations: CDC, Centers for Disease Control and Prevention; NHLBI, National Heart, Lung, and Blood Institute; PI, principal investigator; QALY, quality-adjusted life-year. [A text description of this figure is also available.]
The programs are currently supported by CDC and previously were jointly funded by NHLBI. We do not consider participation costs incurred by clinical laboratories, manufacturers, and research funding agents because participation in the programs is voluntary.
The fundamental activities of the programs are to define reference methods and maintain reference materials for total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein (LDL) cholesterol, and triglycerides. CDC uses a standardized testing protocol on well-characterized and uniform serum materials to eliminate potential reference bias and allow program participant results to be compared directly to the CDC reference results. The programs maintain a set of frozen serum pools that exhibit a wide range of lipid concentrations. Long-term maintenance of these pools is essential to ensure that reference values of these samples do not drift over time.
Using the reference measurement procedures and materials, the LSP conducts standardization of clinical laboratories involved in epidemiologic and clinical research. Establishing a long-term, accuracy-based reference allows results to be compared across different laboratories and over time, which is necessary when conducting multicenter clinical trials; comparing lipid measurement values to past values, such as the baseline period in clinical and epidemiologic research; or comparing lipid measurement values across clinical and epidemiologic research studies. Recommended accuracy goals for lipids and lipoprotein tests, which include both bias and imprecision, have been developed by the National Cholesterol Education Program (11-13). These accuracy goals are based on results obtained from the LSP.
The CRMLN uses the standardized reference methods and materials to certify a network of reference laboratories that seek to replicate the accuracy of the CDC laboratory. In turn, this network of laboratories certifies participating manufacturers and clinical testing laboratories. By calibrating manufacturers’ equipment and testing methods against the CDC reference standards, the CRMLN increases the accuracy of all tests conducted using these supplies, even for clinical laboratories that do not participate in the program. This system allows for accurate comparison of test results to the clinical practice guidelines established by the Adult Treatment Panel III (14).
The programs’ inputs, activities, and participants are intended to produce the following short-term outcomes:
The short-term outcomes — in combination with nonprogram factors — lead to the following medium-term outcomes for patients and health care providers: increased cholesterol awareness, better practice patterns, improved diet and exercise, better drugs, and improved diagnosis of patients with high cholesterol.
The medium-term outcomes combine to produce better cholesterol control, which improves patient health outcomes in the long term by reducing medical events and lowering rates of cardiovascular disease and death. The true benefits of the lipid standardization programs arise from improvements in these long-term patient outcomes.
It is difficult to quantify precisely the effect of the lipid standardization programs on these short-, medium-, and long-term outcomes. For most of the outcomes, standardization of lipid measures is a prerequisite that can support and promote — but does not by itself guarantee — improved public health outcomes. For example, standardization supports clinical trials of new cholesterol-lowering therapies, but development of new therapies also depends on research and development efforts, technologic breakthroughs, and careful clinical testing.
Because we cannot directly attribute outcome changes to program operations, our approach is to investigate improvements in each short- and medium-term outcome during recent years. We discuss qualitatively how the standardization efforts of CDC programs may have facilitated the improvement, but we do not attempt to estimate precisely the share of each improvement that is attributable to the programs. We also do not place a dollar value on the benefits of improvements in short- and medium-term outcomes because the true benefits to patients are associated with improvements in long-term outcomes.
To determine the improvements in long-term outcomes, we applied previous estimates of the change in heart disease deaths between 1980 and 2000 that was attributable to treatment with statins and the overall reduction in total cholesterol during the period. Ford et al (4) and Capewell et al (5) estimated that these cholesterol-related changes prevented or postponed more than 111,000 deaths and saved 1.35 million life-years in 2000 (Table 1).
We considered alternative assumptions about the share of deaths prevented or postponed and life-years saved that were attributable to the lipid standardization programs. We asked experts to estimate the percentage of lipid reduction during the period that was attributable to the lipid standardization programs. The 4 experts work on cardiovascular disease in various settings (1 in a university hospital, 2 in private clinical laboratories, and 1 in the National Institutes of Health). The experts were asked to base their estimates on information on the reduction in CHD deaths between 1980 and 2000 and the estimate (4) that 24% of the reduction was due to lower cholesterol levels. They were told that lipid standardization was potentially one of many factors contributing to lower lipid levels. The experts’ median estimate of the share of lipid reduction attributable to lipid standardization was 5%, but the estimates ranged widely (from 2%-3% to >50%). We also considered more conservative estimates of 0.5% and 1%.
To estimate the dollar value of improvements in life expectancy, we applied alternative estimates of the value of a life-year gained. Setting a dollar value on life-years gained is controversial. In the health economics literature, a value of $50,000 per quality-adjusted life-year (QALY) is sometimes used to assess the cost-effectiveness of interventions, but the conceptual basis for this benchmark is debatable (15). A recent study suggests that society’s willingness to pay for health improvements is at least $113,000 per QALY in the United States (16). For regulatory purposes in cost-benefit analyses of environmental issues, the Environmental Protection Agency (EPA) sets the value of a statistical life-year at $300,000. The EPA estimate is based on an estimate of $4.8 million in 1990 dollars (17) for 1 statistical life that was calculated using wage differentials for risky jobs in the labor market. To convert this value into a value for a statistical life-year, we multiplied $4.8 million by 1.49, the gross domestic product inflator for 2008 relative to 1990. We assumed that the resulting value of a statistical life-year in 2008 represented the net present value of a stream of constant statistical life-year payments received over 40 years (the approximate remaining life expectancy of a 45-year-old adult) with a real discount rate of 3%. Solving for the value of a statistical life-year yields a value of $300,000 per life-year.
We calculated the dollar benefits of the life-years gained attributable to the lipid standardization programs under alternative assumptions about the life-years attributable to the LSP and CRMLN and the value of a life-year gained. We then compared the dollar benefits of the programs to the cost of the LSP and CRMLN in fiscal year 2008, $1.7 million.
As detailed in the Appendix, we found suggestive evidence linking the LSP and CRMLN to improved short- and medium-term outcomes. Program data indicate that laboratories participating in the programs achieve high levels of accuracy. This accuracy supports standardized epidemiologic results, standardized clinical trials, and standardized testing methods used by clinical laboratories, which can lead to improved test accuracy.
Assuming the median expert panel estimate of 5% of the cholesterol-related benefits attributable to the programs and a value per life-year of $113,000, the benefits attributable to the programs are estimated to be $7.6 billion (Table 2). Assuming the most conservative estimates (0.5% of the cholesterol-related benefits attributable to the programs and a $50,000 value per life-year), the benefits attributable to the programs are estimated to be $338 million annually.
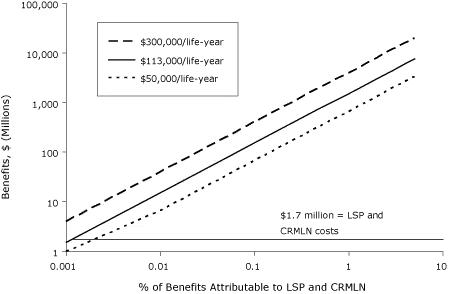
We conducted a sensitivity analysis to examine how the estimated benefits change under alternative assumptions about the percentage attributable to the LSP and CRMLN (Figure 2) in comparison to this cost. Both the percentage attributable and the benefits and costs are presented using logarithmic scales to preserve the true linear relationship between the benefit and the percentage attributable and to allow the benefits and costs to be shown in the same figure (otherwise, the benefit at 5% attributable would completely dwarf the cost of the programs). Even assuming that the LSP and CRMLN are responsible for only 0.01% of the improvement in life-years attributable to cholesterol-related factors, the benefits of the programs substantially exceed their costs.
Figure 2. Benefits of life-years gained from the Lipid Standardization Program (LSP) and Cholesterol Reference Method Laboratory Network (CRMLN). Cost of the programs was $1.7 million per year. [A tabular version of this figure is also available.]
Our estimates suggest that the benefits of CDC’s lipid standardization programs greatly exceed their costs. Deaths from heart disease fell dramatically between 1980 and 2000 (2,3), and this reduction has driven improvements in overall life expectancy. The improvement in life-years has high dollar value. A significant share of the improvement in heart disease deaths is due to cholesterol-related factors, including the overall reduction in total and LDL cholesterol and the use of statin drugs for secondary and primary prevention (4,5). To the extent that some of the improvement in these cholesterol-related factors is due to CDC’s lipid standardization programs, the programs have large dollar benefits because the overall dollar value of the increase in life-years from heart disease — and the share of the increase that is attributable to cholesterol-related factors — is so large. Put another way, the overall benefits of cholesterol reduction are so large that there is plenty of credit to go around to lipid standardization programs and other factors (eg, research and development efforts, technological breakthroughs, careful clinical testing) affecting cholesterol. Even if the LSP and CRMLN receive only a small share of the credit, the programs’ benefits exceed their costs.
Our analysis has several potential limitations. First, our estimates could implicitly overestimate the value of the improvements in life expectancy stemming from reductions in heart disease deaths; however, this does not appear to be the case. Improvements in heart disease deaths are clearly documented in national life expectancy and cause-of-death data. Less evidence exists on the value of this improvement, but a study by Murphy and Topel (18) provides context for our estimates. They estimated that the reduction in deaths from heart disease has increased the value of life by about $1.5 trillion per year since 1970. The Capewell et al study (5) — which is the basis for our estimates — found that 3.15 million life-years were gained in 2000 from all reductions in heart disease deaths between 1980 and 2000. When this gain is valued at $50,000, $113,000, and $300,000 per life-year, the total benefits in 2000 would be $155 billion, $350 billion, and $930 billion, respectively. Thus, the overall benefit from reduction in heart disease deaths given by Murphy and Topel is even greater than the underlying heart disease benefit in our analysis.
Second, our analysis could attribute too much of the gain in life-years resulting from reductions in heart disease deaths to cholesterol-related factors. We relied on studies by Ford et al (4) and Capewell et al (5), which appear to provide the most comprehensive decomposition of the gain in life-years that are attributable to specific factors.
Third, our estimate depends on the share of lipid reduction that is attributable to the lipid standardization programs, and this parameter was not precisely measured. Although the parameter was based on the opinion of experts familiar with the programs, these experts noted that the parameter was difficult to estimate. Even when we included more conservative parameters, the benefits attributable to the programs were still sizeable. Because this is probably the most important potential limitation of our study, it is worth considering additional alternative estimates. The sensitivity analysis shows how the benefits change with the percentage attributable to the LSP and CRMLN for values ranging from 0.001% to 5%. Even when the LSP and CRMLN are responsible for a smaller share of the reduction in life-years attributable to cholesterol-related factors than our expert panel estimated, the benefits of the programs substantially exceed their costs.
Fourth, our estimate of the benefits attributable to the programs is based on the estimated effects of the programs on cholesterol between 1980 and 2000. It is not clear whether standardization would suffer today and in the future if the LSP and CRMLN ceased to exist. One might expect that test values would drift away from true values over time, but it seems unlikely that bias levels would return to their 1980 levels. This limitation can be assessed using Figure 2. Suppose that 1% of the improvement in cholesterol-related factors is due to LSP and CRMLN effects between 1980 and 2000. If 10% of this improvement would be lost if the programs ceased to exist, then the lost benefit would equal 0.1% of the overall cholesterol-related effects. The programs’ benefits would still substantially exceed their costs.
Fifth, our estimates of the improvements in heart disease deaths that are attributable to cholesterol-related factors are based on studies for the period between 1980 and 2000. If more recent data were available, the number of life-years saved by cholesterol-related factors would likely increase because heart disease death rates have continued to fall since 2000.
Sixth, assigning a dollar value to life-years saved is controversial, and when a value is assigned, debate remains about the actual value to set. Nevertheless, the estimated benefit from the lipid standardization programs remains high even if life-years are valued at $50,000 per year.
Finally, our analysis does not include health care cost offsets or increases associated with the reduction in heart disease deaths. In principle, it might be possible to model spending on heart disease for individual patients; however, the level of modeling necessary is beyond the scope of this study.
This is the first study attempting to quantify the benefits of CDC’s lipid standardization programs. At least 1 study has assessed the benefits of improving the accuracy of other clinical tests. Gallaher et al (19) estimated that systematic errors on calcium tests could increase the costs of follow-up testing and procedures by $60 million to $199 million per year. Although that study applied different methods and examined a different test than our study, it provides support for our general finding that improving test accuracy may have substantial financial benefits.
As noted in the introduction, the NHLBI discontinued its funding of the LSP in 2008, raising questions about the program’s future. Our estimates provide evidence of the benefits and costs of the CDC lipid standardization programs that may help policy makers decide whether to continue funding the programs.
This study was funded through a cooperative agreement between CDC and the NACDD, which contracted with RTI International. Mary M. Kimberly and Gary L. Myers from CDC provided helpful information on the LSP and CRMLN. We acknowledge the expert estimates of the LSP- and CRLMN-attributable portion of the reduction in cardiovascular death rates offered by members of the Cardiovascular Biomarker Standardization Steering Committee and other public health experts. Steven Couper, from RTI International, contributed to the Appendix.
Corresponding Author: Thomas J. Hoerger, PhD, RTI International, 3040 Cornwallis Road, PO Box 12194, Research Triangle Park, NC 27709. Telephone: 919-541-7146. E-mail: [email protected].
Author Affiliations: John S. Wittenborn, RTI International, Research Triangle Park, North Carolina; Walter Young, National Association of Chronic Disease Directors, Golden, Colorado.
|
|
|
|
|
|
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Privacy Policy | Accessibility This page last reviewed March 30, 2012
|
|