|
|
||||||||
|
|
| Home |
Volume 8: No. 6, November 2011
Suggested citation for this article: Jue JS, Metlay JP. Web-based health resources at US colleges: early patterns and missed opportunities in preventive health. Prev Chronic Dis 2011;8(6):A138. http://www.cdc.gov/pcd/issues/2011/nov/10_0236.htm. Accessed [date].
PEER REVIEWED
Introduction
Web-based health resources on college websites have the potential to reach a
substantial number of college students. The objective of this study was to
characterize how colleges use their websites to educate about and promote health.
Methods
This study was a cross-sectional analysis of websites from a nationally representative sample of
426 US colleges. Reviewers abstracted information about Web-based health resources from college websites, namely health information,
Web links to outside health resources, and interactive Web-based health programs.
Results
Nearly 60% of US colleges provided health resources on their websites, 49% provided health information, 48% provided links
to outside resources, and 28% provided interactive Web-based health programs. The most common topics of
Web-based health resources were mental health and general health.
Conclusion
We found widespread presence of Web-based health resources available from various delivery modes and
covering a range of health topics. Although further research in this new modality is warranted,
Web-based health resources hold promise for reaching
more US college students.
In 2008, more than 18 million people in the United States were enrolled in college (1), most of whom were young adults aged 18 to 25 years. These young adults are in a unique developmental stage, transitioning to autonomy in decision making and independently developing behavior patterns (2), in particular health behaviors, that they will often continue throughout their lives (3).
Health and disease prevention are often not a priority of young adults. However, when seeking health information, they most often use the Internet, citing accessibility, availability, privacy, and confidentiality as reasons for preference over traditional sources (4). They most often use search engines to seek out health information online (5,6), even though this is not the most efficient way to access health information (7). Young adults experience difficulty in assessing the reliability and quality of information found online (4,8-10). In 1 survey, 90% of college students found college medical center staff to be a credible source for health information compared with other sources (4). No study looks specifically at youth attitudes and behaviors around Web-based health resources on college websites. Yet, given that college student health seeking occurs primarily on the Internet and the most believable source of health information is perceived to be local student health center staff, providing health resources on local college websites may be an effective way to educate and promote health in young adults.
The objective of this study was to characterize how colleges use their websites to educate about and promote health. We describe the presence of various Web-based health resources on college websites. We assessed both the breadth of health categories covered and also the variety of Web-based modes of delivery, which included Web-based health information, links to outside health resources, and interactive Web-based health programs. As a secondary objective, we investigated the hypotheses that the size of the college, public versus private school status, health professional school affiliations, and presence of student health services and health professionals increase the likelihood of health resources being present on college websites.
We conducted a cross-sectional analysis of websites from a nationally representative sample of US colleges. Eligibility criteria included 1) being an accredited 2-year or 4-year bachelors, associate, or trade school degree-granting institution; 2) having at least 1 physical campus located in the United States; 3) having an institutional website; and 4) currently enrolling students. We excluded colleges that were online only, institutions that were graduate-level only, and colleges whose websites were not accessible (ie, password protected). The colleges were selected from the 2009 Higher Education Directory, a comprehensive database of all higher education institutions in the United States (Higher Education Publications, Reston, Virginia). Twelve strata were created based on 1) geographic region (Northeast, South, Midwest, and West) and 2) student body size, including graduate students where applicable (small, <5,000; medium, 5,000-9,999; large, ≥10,000). We randomly selected 30 to 33 colleges from each strata (n = 385 total). We also oversampled 4-year colleges, randomly selecting 8 to 10 four-year colleges from the 12 strata (N = 100). Thus, the final sample included a total of 485 colleges out of a total of 3,506 eligible institutions. Of the 485 colleges, 59 were excluded, and 426 eligible colleges were included in the final sample.
From February 1, 2009, through April 30, 2009, 2 reviewers (ie, abstractors) abstracted data from college websites by using a standardized abstraction tool (Appendix A). Abstractors visited colleges’ official websites as listed in the 2009 Higher Education Directory. In addition to the college main website, reviewers also abstracted data from college student health services and counseling websites (when available). Abstractors were instructed to search for key terms (Appendix B) and look through relevant links from both the main college website and the student health services websites, if applicable. All data collected were in the domain of the college website and did not include student personal or nonaffiliated student group websites. There was no limit to the number of separate websites that could be visited for data collection from each college. To assess interrater reliability, the 2 reviewers both abstracted a 10% overlap of websites. Interrater agreement between abstractors was assessed, and we calculated the Κ statistic for the presence of health information and interactive Web-based health programs (Κ = 0.8 for both). A third reviewer resolved discrepancies between the 2 primary reviewers by examining the websites of those colleges. We held regular meetings with reviewers to discuss questions, issues, and discrepancies.
The primary measure of interest was the presence of Web-based health resources on college websites. The study was designed to assess both the breadth of health categories covered and also the variety of Web-based modes of delivery. We identified 4 major health categories: 1) general health, 2) reproductive and sexual health, 3) substance abuse, and 4) mental health. Each health category was further subdivided into specific content areas (eg, asthma, depression). The categories and content area in each were based in part on the critical health objectives (11) for young adults determined by the Centers for Disease Control and Prevention (CDC) as part of Healthy People 2010 (12). Also identified were 3 Web-based health delivery modes, including 1) direct health information provided directly on websites, 2) outside Web links to other health-related websites, and 3) interactive Web-based health programs. Direct health information was defined as specific information about a health topic or disease that detailed content such as epidemiology of the illness, symptoms, diagnosis, and treatment. Simple listing of the availability of illness-specific services provided did not count as health information. For example, a website describing signs, symptoms, and treatment of chlamydia infections would be considered health information. However, a website merely stating that their student health clinic provided services for chlamydia did not count as providing health information. Outside Web links were defined as Internet links that brought a user from the college website to a noncollege website that provided health information or health-related resources. An interactive Web-based health program was defined as an interactive program accessed on the Internet that addressed a health topic. Though interactive Web-based health programs are neither exclusive of nor necessarily a subcategory of health information, significant overlap exists. The difference from health information was the interactive component, such as an online assessment, a program or file download (eg, podcast), or assessments that were evaluated (eg, submit a survey by e-mail for evaluation).
We collected data on only institutional characteristics as reported in the 2009 Higher Education Directory; these were school name, location, website address, enrollment size, 2-year versus 4-year college, and public versus private status. We collected data on additional institutional characteristics from the college website; these included the presence or absence of campus student health services, counseling services, and staffing, including nurses, health educators, midlevel providers, counselors, and physicians, and affiliations with medical, nursing, and public health schools or programs. Student health services and counseling services are health services or centers focused on students of that college. They need not be physically on campus, but they must be more than an affiliation with or referral to outside health care providers. We determined staffing at student health services and counseling services from website listings on the basis of title and degree.
To generate a final data sample reflective of the population of eligible US colleges, all analyses were weighted by the inverse sampling probability for each sampling strata. The weighting accounted for both the strata and the oversampling. We calculated descriptive statistics of the sample and prevalence of each health resource along with binomial confidence limits. All analyses were conducted by using Stata version 10 (StataCorp College Station, Texas). To assess the association between institutional characteristics and the presence of each Web-based health resource by health category, we conducted weighted logistic regressions by using the Stata survey command. The outcome variables were the presence versus absence of various health categories of Web-based health resources (eg, Web-based resources on mental health), while the predictor variables were the institutional characteristics (eg, presence of student health services). We created final adjusted models by using all institutional characteristics and backward selection (P < .1) to identify independent predictors for each of the 4 health categories and also each of the 3 delivery modes. A priori, we decided to force certain institutional characteristics into the model because we believed they were important, including public or private status, 2-year or 4-year status, and enrollment size. The study was determined to be exempt from institutional review by the human subjects subcommittee at the University of Pennsylvania.
Most colleges were public, small (<5,000 students), and 4-year, findings that were consistent with other estimates (Table 1). We derived weighted characteristics of US colleges from the study sample. Most (77%) colleges had some form of student health services available, with a range of health care providers listed on staff.
Colleges with health educators, 4-year colleges, and large colleges were more likely to provide Web-based health resources in all health categories than were 2-year colleges (Table 2). More colleges provided direct health information in general health (24%), followed by mental health (18%) (Table 3). Of all colleges, 58% provided at least 1 of the 3 modes of delivery of Web-based health resources (direct health information, interactive Web-based programs, and outside links) on their websites for any health topic. Specifically on their websites, 49% provided health information, 48% provided links to outside health resources, and 28% provided interactive Web-based health programs. Sixty-eight percent of colleges with student health services, compared with 22% of colleges without student health services, had some Web-based health resources. Of those providing any Web-based health resources, 76% covered general health topics, 55% covered reproductive and sexual health, 65% covered substance abuse, and 82% covered mental health topics.
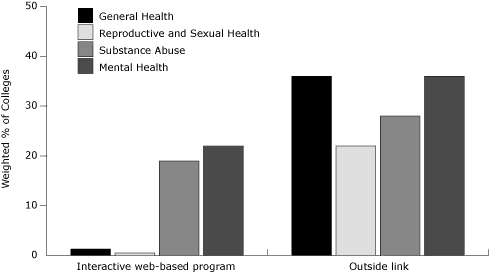
Overall, 48% of colleges provided Web links to outside health resources. Mental health (36%) and general health (36%) were provided most often (Figure). In each health category, links to outside health resources were more prevalent than either direct health information or interactive Web-based health programs provided on college websites. Of the 51% of colleges that did not provide health information directly on their websites, only 17% provided links to outside resources as an alternative. However, of those that did not provide direct health information on mental health, 31% provided links to outside mental health resources.
Figure. Percentage of US colleges with Web-based health resources, by delivery mode and category, February-April, 2009. [A tabular version of this figure is also available.]
The highest percentages of interactive Web-based health programs were in the areas of mental health (22%) and substance abuse (19%). The most common interactive Web-based health programs for mental health were for stress and anxiety (93%). For substance abuse, the most common were for alcohol use (30%). Tobacco use cessation via interactive Web-based health programs was observed at only 1.2% of colleges overall. Similarly, interactive Web-based health programs in the areas of reproductive health (0.5%) and nutrition and weight management (0.4%) were identified in few college websites.
The breadth of health information covered varied substantially by college, the highest percentage of schools providing information for any specific, single topic was only 14.8%. More colleges provided links to outside health resources than provided direct Web-based health information or interactive Web-based health programs on their websites. Interactive Web-based health programs were notably absent for general health and sexual and reproductive health topics and more prevalent for substance abuse and mental health topics.
Mental health had the most overall Web-based health resources on college websites and was the topical category with the most interactive Web-based health programs, specifically programs addressing stress and depression. These findings may reflect both an increase in mental health needs in general and a growing recognition of the need to address behavioral health in young adults. Studies show that though approximately 15% of college students either report a diagnosis of or have symptoms consistent with a diagnosis of depression (13,14), most do not receive treatment (15). Web-based mental health programs may be particularly appealing to young adults, as they help overcome barriers to treating mental health: stigma and cost. Such programs can also decrease the financial burden on colleges for providing information, skill-building, and screening for mental health problems. Another reason that may explain the high number of interactive Web-based health programs in mental health may be related to market forces. One predominant interactive Web-based mental health program that was sponsored by a suicide prevention foundation provided customized interactive Web-based mental health programs to colleges at no cost.
In addition to early prominent patterns, there were also notable absences among particular topical areas. Interactive Web-based health programs addressing tobacco use cessation were uncommon, despite tobacco use being the leading cause of preventable death in the United States (16). Most smokers start before the age of 18 (17), and many arrive at college already addicted to cigarette smoking. However, younger smokers (aged 18-24 y) compared with older smokers (aged 35-64 y) and those who are college educated compared with those who are not are more likely to quit (18,19). Despite this crucial period to target behavior change, less than 10% of colleges in this study offered health information and only 1.5% of colleges offered interactive Web-based health programs related to tobacco use cessation on their websites.
The second leading cause of preventable death in the United States is overweight and obesity due to improper diet and physical inactivity (16). Young adults are the age group at highest risk for weight gain (20-23). Studies also find that when using the Internet to obtain health-related information, adolescents and college students most often seek it in the areas of fitness, exercise, diet, and nutrition (6,8). However, fewer than 10% of colleges provided Web-based health resources related to nutrition or physical activity, and very few nutrition-related interactive Web-based health programs were provided.
The lack of Web-based health resources in tobacco use cessation, nutrition, physical activity, and weight management represent missed opportunities in the prevention of chronic diseases of adulthood. These preventable illnesses are relevant to young adults during the period when many health behaviors are solidified. Targeting behaviors among college students by using Web-based health resources may be a promising avenue to tackle 2 of CDC’s priority “winnable battles,” public health priorities with large-scale impact on health and with known, effective strategies to address them (www.cdc.gov/WinnableBattles).
We also observed a spectrum of college offerings of Web-based health resources. We found a high proportion of colleges with student health services and a related increased likelihood of the presence of online health resources. We also found that small and 2-year colleges were less likely than large and 4-year colleges to provide Web-based health resources, which we theorize relates to limited resources. Yet, most colleges in the United States are small, and approximately a quarter are 2-year colleges. With lower financial barriers to providing Web-based health resources online compared with on-campus health facilities, the use of the Internet may be a low-cost means for colleges to provide health promotion and prevention resources to young adults during their crucial time of health behavior development.
Nearly 60% of colleges in the US use Web-based resources to address health-related topics on their websites. The Internet is playing an increasing role in the interface between patients and providers in health promotion, disease prevention, and management. To our knowledge, this is the first study to characterize how US colleges use their institutional websites to improve the health of their students. Given that our analysis is based on a random sample of colleges, it should generalize to the broader group of all US colleges.
College websites represent a unique subset of websites with potential for high impact given the characteristics of college students. Although few best practices in Web-based health resources targeting college students exist, a few studies of college interactive Web-based health programs suggest significant potential, particularly in behavior modification around substance abuse (alcohol and tobacco) (24,25), sexually transmitted diseases (26), and mental health (27,28). While it appears that colleges with greater resources are more likely to provide Web-based health resources, partnerships with private groups to provide these resources, as described above, may be a practical way for more colleges to maximize their online presence. Further work needs to examine both the quality of Web-based health resource content and also the degree to which different types of college Web-based health resources actually influence health-related behaviors and outcomes.
We acknowledge several limitations to this study. First, our study assumes that college websites are static representations of available resources. However, because of the dynamic and fluid nature of websites, they may be incomplete, incorrect, or not up-to-date at the time they were accessed. Also, we did not assess the content of health information and quality of health resources. Finally, we tested several associations between institutional characteristics and provision of health resources, raising the possibility of chance findings existing with multiple testing.
We found general widespread presence of Web-based health resources of various delivery modes on US college websites. Colleges with certain characteristics related to general resource availability were more likely to provide Web-based health resources. Most US adults spend some time in higher education, so colleges have a unique public health opportunity to provide important preventive health care information via the Internet. Although further research in this new modality is warranted, Web-based programs hold promise for reaching US college students.
During the course of this study, Dr Jue was funded by the Robert Wood Johnson Foundation Clinical Scholars Program at the University of Pennsylvania in partnership with the Department of Veterans Affairs. Dr Metlay was funded by a Mid-Career Patient Oriented Investigator Award (K24-AI073957) at the University of Pennsylvania. Neither funding entities had a role in the design or conduct of the study; collection, management, analysis, or interpretation of the data; nor preparation, review, or approval of the manuscript.
Corresponding Author: J. Jane S. Jue, MD, MSc, ECRI Institute, 5200 Butler Pike, Plymouth Meeting, PA 19462. Telephone: 610-825-6000. E-mail: [email protected]. At the time of this study, Dr Jue was affiliated with the Department of Veterans Affairs, Philadelphia VA Medical Center in Philadelphia, Pennsylvania, and with the Robert Wood Johnson Foundation Clinical Scholars Program at the University of Pennsylvania School of Medicine in Philadelphia, Pennsylvania.
Author Affiliations: Joshua P. Metlay, University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania. Dr Metlay is also affiliated with the Robert Wood Johnson Foundation Clinical Scholars Program, Philadelphia, Pennsylvania.
|
|
|
|
|
|
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Privacy Policy | Accessibility This page last reviewed August 24, 2012
|
|