|
|
||||||||
|
|
| Home |
Volume 3: No. 3, July 2006
Suggested citation for this article: Samuel-Hodge CD, Keyserling TC, France R, Ingram AF, Johnston LF, Davis LP, et al. A church-based diabetes self-management education program for African Americans with type 2 diabetes. Prev Chronic Dis [serial online] 2006 Jul [date cited]. Available from: URL:
http://www.cdc.gov/pcd/issues/2006/
jul/05_0085.htm.
PEER REVIEWED
Introduction
Diabetes self-management education interventions in community gathering places have been moderately effective, but very few studies of intervention effectiveness have been conducted among African Americans with type 2 diabetes. This paper describes a church-based diabetes self-management education intervention for African Americans, a randomized controlled trial to evaluate the intervention, and
baseline characteristics of study participants.
Methods
A New DAWN: Diabetes Awareness & Wellness Network was conducted among 24 churches of varying size in North Carolina. Each church recruited congregants with type 2 diabetes and designated a diabetes advisor, or peer counselor, to be part of the intervention team. Participants were enrolled at each church and randomized as a unit to either the special intervention or the minimal intervention. The
special intervention included one individual counseling visit, twelve group sessions, three postcard messages from the participant’s diabetes
care provider, and twelve monthly telephone calls from a diabetes advisor. Baseline data included measures of weight, hemoglobin A1c, blood pressure, physical activity, dietary and diabetes self-care practices, and psychosocial factors.
The study to evaluate the intervention (from enrollment visit to last follow-up)
began in February 2001 and ended in August 2003.
Results
Twenty-four churches (with 201 total participants) were randomized. Sixty-four percent of the participants were
women. On average, the participants were aged 59 years and sedentary. They had an average of 12 years of education, had been diagnosed with diabetes for 9 years, had a body mass index of 35, had a hemoglobin A1c level of 7.8%, and had a reported dietary intake of 39% of calories
from fat.
Conclusion
A New DAWN is a culturally sensitive, church-based diabetes
self-management education program for African Americans with type 2 diabetes
that is being evaluated for effectiveness in a randomized controlled trial. The
outcomes of A New DAWN will contribute to the literature on community-based interventions for minority populations and help to inform the selection of approaches to improve diabetes care in this population.
Approximately 2.7 million African Americans aged 20 years or older (11.4%) have diabetes, with rates reaching 25% among African Americans aged 65 to 74 and African American women older than 55 (1). Despite the health disparities associated with type 2 diabetes among African Americans compared with whites, relatively few intervention programs have been designed to improve self-management behaviors and metabolic control in this high-risk group. In a recent review of diabetes self-management interventions (2), only one of eight community-based studies published through December 2000 involved African Americans, yet African Americans are almost twice as likely as whites to have diabetes and have two to five times more diabetes complications, including kidney failure, lower limb amputations, and blindness (1). This disparity could be reduced through better self-management behaviors. Diabetes self-management education (DSME) in community gathering places such as churches has been moderately effective and provides opportunities for education that would not normally exist, especially in rural areas (2). Among African Americans, church-based health education and screening programs have effectively facilitated behavior change (3), but only a few reported church-based DSME interventions have targeted African Americans already diagnosed with diabetes (4-5).
We designed a new, culturally sensitive church-based intervention for African Americans with type 2 diabetes to fulfill three main objectives: 1) promote changes in dietary and physical activity behaviors and improve metabolic control, 2) enhance physician-directed outpatient care by providing a community resource to support self-management behaviors, and 3) build churches’ capacity to raise the awareness of diabetes’ impact on the community’s health. The first two objectives are consistent with the model of chronic disease management described by Wagner et al (6), which emphasizes the need for linking the clinical care of patients with diabetes and community support systems for daily disease management. The third objective involves a multilevel intervention — targeting the church as an institution, the community, and the individual. This objective reflects the need for community-based research to integrate opportunities for community capacity building, which would result in communities that have skills and resources at the end of the research period (7,8). This paper describes the intervention A New DAWN: Diabetes Awareness & Wellness Network, the randomized control trial to evaluate the intervention, and baseline characteristics of the churches and study participants.
A New DAWN was a year-long church-based intervention comprising four intervention components for participants with diabetes and two intervention components for the entire church membership. The study to evaluate the intervention (from enrollment visit to last follow up) began in February 2001 and ended in August 2003.
Individual counseling visit
Each enrolled participant was scheduled for a 60-minute individual counseling session that was held at the church and conducted by a registered dietitian. The counseling visit began with brief assessments of 1) dietary habits (using the food-frequency–based Dietary Risk Assessment) (9); 2) psychosocial issues such as stress management, social support, and problem solving; 3) eating patterns (e.g., timing and consistency of meals); and 4) barriers to dietary and physical activity behavior changes. A detailed description of the assessment, educational materials, and counseling strategies has been published elsewhere (10).
Group education sessions
The 12 group sessions held at each church had a basic format and structure. The sequence of sessions was determined by review of standard DSME curricula (11) and a decision to focus on dietary behaviors during the first five sessions. Physical activity and blood glucose self-monitoring were components of each session. Table 1 includes session topics and their associated behavioral and learning objectives. Before each session, participants had their blood glucose level (using the finger-stick method) and blood pressure checked. Participants received feedback on how their blood glucose levels and blood pressure results compared with the American Diabetes Association (ADA) targets and previous entries in the participants’ monitoring log. During the monitoring sessions and the group discussions, participants shared successful strategies they had used to make progress toward goals or began brainstorming ways to make progress during the following weeks. After the monitoring was complete, each session opened with a prayer by one of the participants or the church diabetes advisor (CDA) and an overview of the session’s content by the group facilitator. The educational component of each session was followed by a short (approximately 15-minute) physical activity segment incorporating chair exercises and a tasting of one or two recipes.
A registered dietitian led the first seven group sessions, with the CDA assisting by greeting the participants, distributing session materials, conducting small group activities, and serving food items for tasting. The educational component of sessions eight through eleven was designed to be led by a health care professional (e.g., pharmacist, dentist, social worker, podiatrist) from the community or church who had been invited by the CDA. This approach was used to 1) teach the CDA how to identify and request the services of community health professionals for church-based activities and 2) expose study participants to the expertise of local health professionals who may not be part of their current diabetes clinical care team. The church was given the option to choose the session topic for the last group session; having a potluck meal was also an option.
When designing the group sessions, we incorporated theories of behavior change and adult education (13,14). Table 2 includes a description of the theoretical basis of the intervention component. We also made sure to design small group activities that were appropriate for individuals with limited literacy or those unaccustomed to group education and interactions. Each session was interactive (nondidactic), included visuals and hands-on activities, required little writing in group activities, used a game format for teaching nutrition concepts whenever feasible, and included opportunities for participants to share their successes and struggles with the group during problem-solving discussions. Because one of our main objectives was to change eating practices through changes in food preparation and selection, we asked church members which dishes were common at church food events, selected recipes for healthier versions of each, and tested the acceptability of all recipes before including them in the group sessions. For each session, two recipes, including a printed copy with nutrient analysis, were prepared for tasting.
We limited the physical activity in each session to chair exercises so that participants with physical activity restrictions could participate and focus on demonstrating activities to improve flexibility and strength. Participants who did not have restrictions on their ability to engage in moderate physical activity were encouraged to engage in 30 minutes of other activity (primarily walking) on most days of the week.
CDA telephone calls
When enrolling churches into the trial, we provided each pastor with a flyer describing the personal qualities a CDA should possess and the job-related expectations. After selection by the pastor, the CDAs were trained during 1 month (4 weekly 4-hour sessions) in the areas of motivational interviewing techniques, listening skills, diabetes self-management (with a focus on diet and physical activity), and telephone calls, record keeping, and other administrative responsibilities. The CDA was a peer counselor — a person with type 2 diabetes or who, for at least 2 years, has lived with someone who has diabetes. The CDA contacted participants monthly by telephone and offered support for behavior changes by following up on diet and activity goals, problem solving with the participant, offering information, and providing the participant with community resources.
The first call from the CDA was made after the participant’s individual counseling session with the dietitian, during which dietary, physical activity, and diabetes self-care habits were assessed and participants set their first negotiated goals. A copy of these goals and a list of areas in which behavior changes could be made were sent to the CDA to help guide the telephone calls. This assessment was provided as part of the client profile, which included contact information, selected demographic and physiological data, and perceived barriers to diabetes self-care. With the client profile, the CDA received forms to document each telephone conversation, a journal to document any personal information that would help the CDA remember the important issues for each participant, and 12 conversation guides — one for each call. These conversation guides were designed to give the CDA suggestions on how to prepare for and conduct each participant telephone call.
Postcard messages from health care providers
DSME programs conducted in community settings are seldom coordinated with participants’ clinical care (2). This lack of coordination is a major deficiency in program implementation and an issue we attempted to address with written messages of encouragement from the participants’ diabetes care providers. The postcard messages were designed to reinforce the importance of good clinical care and optimal self-management as essential components of diabetes care.
To design the postcard messages, we conducted focus groups with primary care physicians. During these discussions, we evaluated several suggestions for communicating health care providers’ support of the feasibility and potential impact of A New DAWN. Although health care providers considered their role as “cheerleaders” of positive behavior changes to be important, they emphasized that they did not want the delivery of these messages to require their time or the time of their staff. Therefore, we developed short, encouraging messages and sent them to participants on the providers’ behalf. All messages were fewer than 100 words and addressed general recommendations for physical activity, dietary behaviors, and HbA1c and blood pressure control. We tailored topics to be consistent with goals selected by participants and the overall goals of the study. We sent three postcard messages by mail at approximately 2-month intervals during the first 8 months of the study.
We also designed A New DAWN to offer the entire church community opportunities to become more aware of diabetes prevention and treatment. We used two strategies to accomplish this objective: the Church Health Action Team (CHAT) and church bulletin boards.
CHAT
Instead of simply providing diabetes information to churches, we trained a few church members to lead the effort. Each church identified three or four members (along with the CDA) to form a team that would plan and implement churchwide activities to increase diabetes awareness. CHAT members attended a 3-hour workshop in which they were trained to compile materials for a diabetes resource manual and plan a diabetes and health fair.
A New DAWN church bulletin board
Diabetes information, recipes from each session, and other program materials were displayed on a bulletin board in a high-traffic area of each church. Displays were changed after each group session.
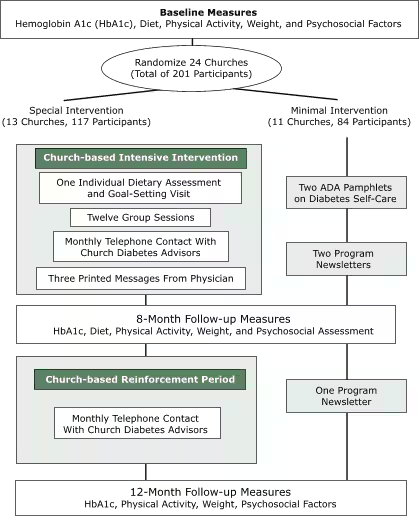
The Figure shows the design of the multisite, randomized controlled trial. After collecting baseline measures, we randomized churches to receive either the special intervention (SI) as described (one individual counseling visit, twelve group sessions, three postcards, and twelve telephone calls) or the minimal intervention (MI). The MI involved a direct mailing to participants of two ADA pamphlets (“Healthy Eating” and “Staying Active”) and three bimonthly newsletters that provided general health information and study updates. In addition, each MI church was offered the intervention materials and an opportunity for the study staff members to conduct one group session at the church to show participants how to use the materials. The study protocol was approved by the institutional review board at the University of North Carolina at Chapel Hill. Before enrollment, written informed consent was obtained from each participant.
Figure. Randomized controlled trial diagram, A New Dawn. ADA indicates American Diabetes Association. [A text description of this chart is also available.]
Recruiting churches and participants
Our participant recruitment approach incorporated findings from a focus group with pastors and other church leaders. At each church, a liaison was identified to facilitate recruitment, and then the congregation was introduced to the program through posters, pamphlets, and pulpit announcements. Congregants who expressed interest in participating (by calling a toll-free number at the research office, sending a card to the research office, or mentioning their interest to the church liaison) were called by a research assistant, who then assessed eligibility and answered questions about the study. Study staff members scheduled an enrollment visit at the church for each interested person and later conducted three telephone interviews to collect additional baseline data.
Study measurements
Physiological measures included HbA1c, weight, and blood pressure. HbA1c was determined from a blood sample collected during enrollment and follow-up visits. Using a standard finger-stick technique, 5 μl of capillary blood was collected into a capillary collection vial (Bio-Rad, Hercules, Calif), which was stored at 4°C. Blood samples were shipped to the Diabetes Diagnostic Laboratory (University of Missouri, Columbia, Mo), where HbA1c was assessed by automated affinity high-performance liquid chromatography on a Primus CLC-330 system (Primus Corp, Kansas City, Mo). Weight was measured with electronic scales (Seca 770, Seca Corp, Columbia, Md). Blood pressure was measured using the Omron HEM-907 automated blood pressure monitor (Omron Healthcare Inc, Bannockburn, Ill) (16,17). Three blood pressure measures were obtained at 60-second intervals, and the average was recorded.
Physical activity was assessed by the ActiGraph monitor (ActiGraph, Shalimar, Fla), a small, uniaxial accelerometer worn on the waist. Several studies have evaluated the validity of the ActiGraph monitor and report satisfactory correlations between the monitor and other measures of physical activity (18-20).
A food frequency questionnaire (FFQ) administered during the first of three telephone interviews was used to assess dietary intake. We selected the Fred Hutchinson Cancer Research Center 12-page FFQ, an instrument that was previously validated in a sample of women that included African Americans (21).
We measured several psychosocial variables to describe the study sample and evaluate potential determinants of targeted behavior changes. (The results will be presented in a future article.) Among the 15 psychosocial constructs measured, 10 were developed or adapted for an African American population from previously validated measures; all new or adapted measures have demonstrated acceptable psychometric properties. Psychosocial measures included church involvement and spirituality, coping styles (22), diabetes and general health status (23,24), perceived diabetes competence (25), perceived stress (26), diabetes problem areas (27) and perceived social and diabetes-related barriers (28), social support (29), familial roles (30), self-efficacy (31), and stages of dietary and physical activity behavior change (32). Most measures were administered during two telephone interviews; the exceptions were measures of perceived stress level and stages of dietary and physical activity behavior change, which were administered in person at the enrollment visit.
Sample size, randomization, and statistical methods
Sample size calculations were based on the following assumptions for the primary study outcome, which was the comparison of HbA1c levels between treatment groups at the 8-month follow-up: a two-sided test (α = 0.05); a power of 80% to detect a mean difference of 1% in HbA1c levels between groups; a cluster (church) randomization with an intraclass correlation (ICC) of 0.031 (based on findings in a previous study) (33); and 10 participants per church. Twenty-eight churches (280 participants) were required. However, we were only able to recruit 24 churches and 201 participants. Consequently, with an average of eight participants per church, an observed intraclass correlation for the baseline HbA1c of 0.0064, expected attrition of 10%, and assumptions as noted, our power to detect a 1% difference in HbA1c between groups was 72%.
To prevent contamination between the SI and MI interventions, we randomized each church as a unit. Randomization was stratified by church location (rural or nonrural, as defined by the United States Postal Service) because of presumed location differences in church size, church members, and organization. Using computer-generated random numbers, a statistical consultant prepared a set of sequentially numbered sealed envelopes containing study group assignments. Churches were assigned to a study group after required baseline data (dietary, physical activity, and demographic information) were collected from all participants within a church.
Comparisons of baseline characteristics between study groups controlled for randomization by church were made using mixed-effects models (34). This approach adjusts for correlation among observations from the participants within each church. For skewed non-Gaussian data, we used the Mann-Whitney U test for clustered data (35). In each model, the baseline characteristic being compared was the dependent variable; the intervention group was treated as a fixed effect, and the church was treated as a random effect. SAS software (SAS Institute, Cary, NC) was used for the analysis, and all reported P values are two sided.
Of 118 churches initially contacted, 30 agreed to participate, and of those, 24 enrolled the required minimum number of participants. The 24 churches were randomized to the SI or MI group — 13 churches (117 participants) to the SI group and 11 churches (84 participants) to the MI group. Comparisons of selected characteristics of churches by intervention group assignment (i.e., SI or MI) revealed no significant group differences according to denomination (e.g., Baptist vs non-Baptist), number or age distribution of active members, age or education of pastor, or previous (i.e., in past 2 years) participation in research projects.
Baseline characteristics of participants are shown in Table 3. All but 1.5% (n = 3) of participants identified themselves as African American (data not shown). On average, participants were 59 years of age, had been diagnosed with diabetes for 9 years, and had completed the 12th grade; 64% were women. Approximately half of the participants were married or living with a partner and were currently employed; 45% had total household incomes of less than $30,000, and 8% had no health insurance. Although only about 8% of participants were current smokers, 75% were being treated for hypertension, and 19% had known coronary heart disease. Self-reported dietary intake showed that 39% of total calories came from fat, with 12% coming from saturated fat. The mean HbA1c was 7.8%, and the mean body mass index (BMI) was 35. Overall, participants were sedentary and participated in minimal minutes per day of moderate or vigorous physical activity.
Information on participants’ diabetes-related medical care and self-care behaviors is presented in Table 4. Although participants reported having frequent appointments with their diabetes physician (an average of 4.6 appointments per year), only 17% had received dietary counseling on two or more occasions during the previous year. Approximately 75% of participants were taking oral diabetes medications, 29% were taking insulin, and 12% were taking no diabetes medication. Almost all (96%) participants had been screened for high blood cholesterol, with 33% taking cholesterol-lowering medication and 50% taking aspirin regularly. No significant differences were found between groups.
Although many reported consuming a low-cholesterol and low-fat diet, less than a third said they were following a diet to lose weight or following a diet for diabetes on 5 to 6 days per week (data not shown). Approximately 85% of participants measured their blood glucose levels at home; about 75% did so once per day. Overall, participants in both treatment groups were similar, although the SI participants were significantly younger.
A New DAWN is a church-based DSME intervention designed to be culturally appropriate and consistent with current behavioral and educational approaches for diabetes self-management. This intervention not only includes culturally sensitive features in design, delivery, and evaluation but also incorporates features that address the psychosocial and contextually relevant influences on health behaviors (36,37). Although they are not well-defined in the literature, we believe the latter factors are reflected in A New DAWN’s focus on 1) organizing education around the “church family” (with family members included as study participants and invited as guests to the group sessions); 2) life experiences as a source of experiential knowledge through the CDA and group interactions and sharing during sessions; 3) using CDAs as cultural translators and diabetes advocates; and 4) measuring psychosocial factors using instruments that were developed and tested for cultural relevance and linguistic appropriateness. Special attention was given to the conceptualization and measurement of psychosocial factors in this group. Surveys were developed or adapted for cultural and linguistic appropriateness and tested for construct validity. A New DAWN was designed and implemented with the collaboration of researchers and the church community, making it a culturally relevant intervention capable of producing useful contextual information (38) to enhance DSME research in this setting.
Only one other church-based DSME intervention for African Americans tested by a randomized controlled trial design has been published (5), so A New DAWN will provide important information related to the design, implementation, and effectiveness of church-based diabetes interventions. The Patient-Owned Enhanced Education Regimen (POWEER) intervention (5) was conducted in four large urban churches (with 109 participants) in the northern United States. In contrast, results from A New DAWN (with 201 participants) will provide information about a southern, more rural population in 24 churches of varying membership size. In addition, results from both trials will allow evaluation of different aspects of the church environment on program acceptability and outcomes. It may be important to have information on how programs designed with the church as a social unit, with existing social relationships among participants who share a common church experience (A New DAWN), differ from those with the church as a community gathering place for intervention activities (POWEER). Data from POWEER indicate that attendance for the intervention group sessions was best among participants recruited from the church (5).
A review of A New DAWN’s design and the sample of enrolled churches reveals some limitations as well as potential applications. First, it was challenging to recruit churches into the trial — only 25% of churches contacted agreed to participate, and 20% of those who agreed were not randomized because they did not recruit enough participants, pastors changed their minds about participation, or leadership changed. Some reasons that churches may not have wanted to participate include 1) not wanting to add a new program because of numerous existing outreach efforts (39); 2) lack of positive experiences with research participation (with only 22% of our sample having participated in research projects during the last 2 years); and 3) considering diabetes to be a medical condition best handled by health care professionals in a clinical setting. If the church is to play an important role in supporting self-management behaviors for African Americans (within the framework of chronic disease management), then the success of programs such as A New DAWN may increase the community’s awareness of how churches can play a role in improving diabetes care. Second, the role of the CDA in interventions such as A New DAWN will need additional evaluation to assess its potential in facilitating church support systems for patients with diabetes.
Participants recruited from churches for A New DAWN differed in important ways from participants in other clinic-based diabetes interventions (10,33,40) conducted in central North Carolina. A larger proportion of A New DAWN participants had private health insurance, and the participants had higher educational levels and higher incomes than participants in studies by Rothman et al (40) and Keyserling et al (10,33). Moreover, A New DAWN participants were less likely to be using insulin when they enrolled, and they had lower HbA1c levels than participants in the other studies. The baseline characteristics that were similar among participants in all of these studies include age, sex, duration of diabetes, and BMI.
The characteristics of participants who volunteered for A New DAWN limit how much we can generalize the study outcomes to other groups of African Americans. Other limitations include 1) a study design that does not allow for evaluation of specific program components on outcome variables (e.g., the independent effects of the CDA or physician messages on metabolic or behavioral changes) and 2) outcome measures that focus primarily on people with diabetes, so the impact of intervention components such as the CHAT, church bulletin board, and CDA on behaviors and awareness of diabetes among church members are not adequately assessed.
To address the high prevalence of diabetes among African Americans, more research is needed to develop effective community-based programs. Eliminating the health disparities associated with diabetes requires culturally appropriate and effective interventions that address the individual’s role in self-management and the community’s role in supporting self-care. In an attempt to meet this need for effective interventions, we developed A New DAWN as a culturally appropriate program that incorporates salient aspects of the chronic disease model (6). The outcomes of A New DAWN will contribute to the literature on community-based interventions for minority populations and help to inform the selection of approaches to improve diabetes care in this population.
This study was supported by cooperative agreement number U48/CCU409660 with the Centers for Disease Control and Prevention, Special Interest Project #22PR-99. We are indebted to the church leadership and congregants of the 24 North Carolina churches whose involvement made this study possible.
Corresponding Author: Carmen D. Samuel-Hodge, University of North Carolina at Chapel Hill, Department of Nutrition, Schools of Medicine and Public Health, CB #7426, 1700 Airport Rd, Room 246, Chapel Hill, NC 27599-8140. Telephone: 919-966-0360. E-mail: [email protected].
Author Affiliations: Thomas C. Keyserling, University of North Carolina at Chapel Hill School of Medicine, Chapel Hill, NC; Renaé France, Allyson F. Ingram, Larry F. Johnston, Lisa Pullen Davis, Gwen Davis, Anne S. Cole, University of North Carolina at Chapel Hill, Center for Health Promotion and Disease Prevention, Chapel Hill, NC.
|
|
Tables
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
DASH indicates Dietary Approaches to Stop Hypertension (12).
aOpportunities for self-monitoring blood glucose and blood pressure, physical activity, and tastings were behavioral components of each session.
bPersonal health habits include foot, skin, and dental care.
cChurch members decide on session topic or to have social event with potluck.
|
||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
SI indicates special intervention; MI, minimal
intervention; MET, metabolic equivalent; IQR, interquartile range.
aAll data and comparisons between groups are adjusted for study design (randomization of churches to SI or MI).
bPercentages equal greater than 100% because some participants had more than one type of health insurance.
cPhysician diagnosis of myocardial infarction or angina or history of percutaneous intervention for coronary heart disease or coronary artery bypass surgery.
dMyocardial infarction or sudden death of unexplained cause in father or brother before age 55 years or mother or sister before age 65 years.
eFor minutes of physical activity per day, medians and IQR are crude data; however, P values for these comparisons are adjusted for study design (randomization by church).
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
SI indicates special intervention; MI, minimal intervention.
*URLs for nonfederal organizations are provided solely as a service to our users. URLs do not constitute an endorsement of any organization by CDC or the federal government, and none should be inferred. CDC is not responsible for the content of Web pages found at these URLs.
|
|
|
|
|
|
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the authors’ affiliated institutions. Use of trade names is for identification only and does not imply endorsement by any of the groups named above.
Privacy Policy | Accessibility This page last reviewed March 30, 2012
|
|