 |
|
||||||||
|
|
| Home |
Volume 1: No. 1, January 2004
Suggested citation for this article: Smith LT, Johnson
DB, Beaudoin S, Monsen ER, LoGerfo JP. Qualitative assessment of participant
utilization and satisfaction with the Seattle Senior Farmers' Market
Nutrition Pilot Program. Prev Chronic Dis [serial online] 2004
Jan [date cited]. Available from: URL: http://www.cdc.gov/pcd/issues/2004/
jan/03_0010b.htm
PEER REVIEWED
Introduction
The Seattle Senior Farmers' Market Nutrition Pilot Program delivered fresh
fruits and vegetables to homebound seniors in King County, Washington, from
June through October 2001. A primary objective of the program was to
increase participants' intake of fruits and vegetables. A qualitative study
was conducted to examine the impact of the program on participating
homebound seniors.
Methods
Semi-structured interviews were performed with 27 participants in their
homes to identify benefits and barriers they encountered and to measure
their use and sense of satisfaction with the program.
Results
Analysis of the transcribed interviews revealed several common themes:
Conclusion
Program success was rooted in the multiple ways the program addressed
potential barriers and reinforced behavioral intent.
Older adults, compared to younger adults, tend to eat more servings of fruits and vegetables, yet many older adults do not consume the recommended 5 or more daily servings (1). Approximately 65% of older adults in Washington State consume less than the recommended 5 servings of fruits and vegetables per day (1).
There are several potential barriers to adequate consumption of fruits and vegetables among older adults (2,3). Physical and cognitive disabilities may prevent shopping and cooking. Dental problems and difficulty chewing and swallowing interfere with eating many foods, especially raw vegetables and fruits. Also, sense of taste can change with aging so that some foods are less appealing or even distasteful. Additionally, the use of medications escalates with aging, and many medications can alter taste, depress appetite, and interfere with digestion (4). Although preference for eating fruit is more prevalent among older compared to younger adults, especially among women (5), lack of financial resources is a significant barrier to healthy eating habits for many older adults (6,7).
From a public health perspective, good nutrition is a significant factor in promoting health and quality of life (8). The outcomes of community-based interventions to increase fruit and vegetable intake have varied considerably (9). More successful interventions have observed increases ranging from 0.5 to 3.7 servings per day. Successful interventions have the following qualities: they are flexible, they are based on a theoretical model, they incorporate feedback from the target audience, they include multiple tactics to communicate and reinforce messages, and their messages specifically address increasing fruit and vegetable intake.
The Food and Nutrition Services of the United States Department of Agriculture (USDA) funded the Senior Farmers' Market Nutrition Pilot Program (SFMNPP) in Washington State in 2001. The purpose of SFMNPP is two-fold: to provide fresh, locally grown fruits, vegetables, and herbs from community-supported agriculture programs to low-income seniors and aid expansion of domestic farmers' markets and community-supported agriculture (10).
Many state Senior Farmers' Market Nutrition projects use voucher systems for qualifying seniors to purchase fresh produce at farmers' markets (11). In Washington State, a unique program was developed to target homebound seniors. From June through October 2001, bags of fresh fruits and vegetables were delivered every other week to homebound seniors who also received their home-delivered (frozen) meals through Seattle Senior Services in Seattle and other locations in King County. The program lasted 20 weeks for a total of 10 deliveries per participant. Each basket contained locally grown, fresh produce including fruits, vegetables, and herbs. Each delivery included a program newsletter that listed items in the bag and described recipes and simple methods of preparation. Newsletters provided information about nutrition, local farmers who grew the produce, SFMNPP collaborating agencies, and volunteer involvement.
The use of both quantitative and qualitative approaches to evaluate the same health promotion program can overcome limitations of either method alone (12). Qualitative evaluation can derive insights directly from the subjects that a program is intended to benefit, and adherence to established standards of qualitative research methodology supports credibility of the research findings (13). Qualitative research is considered to be valid to the extent that the study findings correspond to reality (14). Triangulation is an analytical method used to validate study findings. Through triangulation, qualitative research findings are compared with outcomes obtained by a different method (12), or the qualitative study findings are applied to an existing model that was based on outcomes from a similar but different study. The extent to which the study outcomes fit the existing model lends validity to the study findings.
Brug and colleagues (15) developed a model of fruit and vegetable intake based on qualitative research of adults aged 17 to 45 years who lived in Holland. In this model, behavioral intent strongly correlates with self-efficacy and attitude that, in turn, overcome barriers to fruit and vegetable intake (Figure 1). The model of attitudes, social influence, and self-efficacy (ASE) illustrates how an intervention can address multiple factors that contribute to a person's intention and, in turn, overcome barriers to the target behavior.
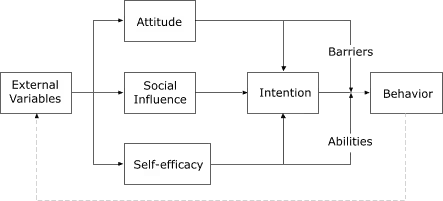
Figure 1.
Model of Psychosocial Determinants of Fruit and Vegetable Consumption.
Adapted from Brug et al (15). Reprinted with permission from Elsevier.
We used certain criteria in determining the quantity of information and the number of interview subjects needed for appropriate and adequate data (16):
In our study, we assumed that SFMNPP participants represented a non-homogeneous sample and thus we would need up to 20 interviews.
The purpose of our study was to interview homebound seniors and identify themes and significant issues regarding participants' experiences with the program. Validity of the study findings was supported by triangulation with the quantitative evaluation of participants' fruit and vegetable intake and by comparison with the ASE model.
The overall study design and methodology were based on the principles of qualitative research and previously published examples of qualitative research applied to health and nutrition studies (14). The procedures of this study are diagrammed in Figure 2. Human subjects approval was obtained from the Internal Review Board of the University of Washington.
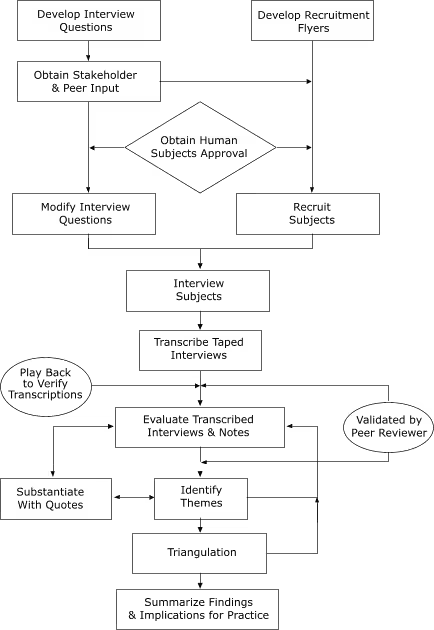
Figure 2.
Procedures for Qualitative Assessment of Seattle Senior Farmers' Market
Nutrition Pilot Program, 2001.
In qualitative research, a directed approach to sampling targets subjects who will be optimally informative and yield rich data (17). In our study, subjects were self-selected. We placed recruitment flyers in produce bags during the fifth cycle of deliveries. A $10 incentive was offered. Volunteers replied by mailing in a preaddressed, postage-paid card or by leaving a telephone voice mail message. We conducted interviews during the sixth through the ninth delivery cycles.
After the first week of recruitment, it became apparent that more individuals volunteered than could be interviewed. We halted further recruitment and selected subjects from the existing list. We based interview subject selections on geographic location so we could include the different areas served in Seattle and King County. We could not base selection on race or age, because that information was not available prior to the interview. We continued program enrollment so that we would have enough subjects to represent the racial, ethnic, and age diversity of homebound participants.
One of the 28 volunteers cancelled the interview. We conducted 27 in-person interviews in subjects' homes. Two subjects declined to have the interview audiotaped, and one session was not taped due to equipment failure.
SFMNPP stakeholders provided input on the design of the interview questionnaire (Appendix). Stakeholders included Senior Services of King County, Public Health-Seattle & King County, King County Area Agency on Aging, Pike Place Market Community Supported Agriculture, and the University of Washington Health Promotion Research Center. The focus was to identify and understand behavior that sustained and/or improved consumption of fresh fruits and vegetables. The questionnaire was pre-tested by mock interview with a nutritionist. The interviews with program participants lasted 20 to 45 minutes. The interview questions were both directed and open-ended so that we could address certain issues and also encourage subjects to bring to mind whatever was important to them (18). Although not specifically asked, many subjects provided information about their health, physical or cognitive disability, and financial ability to purchase fresh fruits and vegetables. Participants were asked about the following areas:
Probing was used to help subjects recall their use of the produce, problems experienced, whether or not they had help with preparing the produce items, other sources of fresh produce for comparing the quality of the produce, and their experiences with the newsletter.
We systematically reviewed written transcripts to identify and substantiate themes relating to participant utilization of the fruits and vegetables and participant satisfaction with the program. The 4 major steps used in data analysis were as follows (19):
As indicated by the flow diagram (Figure 2), the process was iterative. We repeated the same steps with each transcript and for each theme and subcategory, and then we discussed, revised, and applied the findings to the model. The process continued until themes were stabilized and no new themes were generated.
The interview subjects represented the range of gender, age, and race of Seattle Meals On Wheels participants (Table). The diversity of ethnic minorities was less represented. For example, there were no Asian or Pacific Island participants among the interviewees. It is likely that the limited diversity represented by the interview subjects was due in part to the small sample size. In addition, cultural differences may have influenced participants' responses to recruitment.
The interviewer noted the type of housing and whether the person lived alone or with one or more people at the time of the interview. Most of the subjects lived alone (20 out of 27), and the majority lived in public housing, senior housing, or other rental units (15 out of 27).
We taped 24 of the 27 completed interviews. To minimize transcription errors, the tapes were played, transcribed, replayed, corrected, and then replayed to check the corrected transcription. We created headings to capture the variety of topics introduced by the interview responses. In addition, we extracted quotes from the transcripts and organized them according to the following headings:
Analysis led to the identification of themes that we then substantiated by quotes and/or observations from the interview. Four major themes emerged and are presented below.
Theme 1: Utilization of fresh fruits and vegetables
Participants indicated whether they used everything, used everything except
for only one or 2 items, or regularly did not use 3 or more items. All
participants who we interviewed for this study reported that they used most
or all of the fruit items. A 79-year-old female said: "I used it all. I
love vegetables and fruit. I find my health is better when I eat as much as
I can of it."
Since the fruit items could be eaten without cooking, seniors who needed help with chopping and cooking could wash and eat the fruit without assistance. Most of the fruit items (peaches, cherries, apples, Bartlett pears, strawberries, blackberries, and blueberries) were familiar to all the participants. Later in the program, less common varieties such as black pears and Asian pears required identification. Some seniors said that because fruit is expensive, they would not have been able to buy the amount or variety of fruit that they received through the program.
"I love it. I hope it never ends. I know it will, but I just love it. I tell you I couldn't afford to get all of the fruits, like what they put in the basket, I couldn't afford it," said a 65-year-old female.
"I don't think I'd eat that much food if I had to pay for it, it's so expensive. The fruit is so high this year," commented another female, 75 years of age.
Vegetable use varied more than fruit use. Participants who followed special diets or had one or more food restrictions involving fruits or vegetables still used most of the produce they received. For example, one senior who could not eat corn ate everything else and gave the corn to another senior in her building.
We also explored the relationship between utilization of produce and needing help to prepare food. All the participants who had a caregiver reported using all of the produce. A few seniors said that they needed more help and could not manage to prepare some of the produce, especially vegetables that required cooking. However, other participants with physical disabilities found ways to prepare things themselves or get help. It was clear that attitude as well as physical ability affected the outcome of utilizing most or all of the produce items. For example, one senior, a 65-year-old male, was confined to a wheelchair and could not readily use the kitchen. He offered this comment: "I can't cook too well, so I have a neighbor, I share my vegetables with her. She cooks them and shares them with me. That has worked real good."
An initial concern among the stakeholders of SFMNPP in Seattle and King County had been the potential for adverse health effects from the produce. Possible problems included food allergies, food borne illness from eating unwashed or spoiled produce, and drug interactions — for example, the anticoagulant warfarin (also known by the trade name of Coumadin®) may react with vitamin K in dark, green-leaf vegetables. However, participants did not report having any problems. Three seniors reported that they used Coumadin®, but they knew what items they needed to avoid and passed those items on to someone else. Only one person reported possible problems associated with the produce: this individual had a complex medical condition that included immune suppression, intermittent hospital stays, the use of Coumadin®, and the inability to prepare produce that required chopping or peeling. This participant suggested that having half of the produce delivered once a week (instead of a full allotment every 2 weeks) would have allowed her to utilize more of it. Nonetheless, this person knew how to manage her condition and appreciated receiving the fresh produce, none of which she could afford to buy.
Theme 2: Participants' perceived benefits from SFMNPP
Seniors frequently made statements about how they appreciated the variety
and quality of the home-delivered fresh produce. Many of the seniors related
that through SFMNPP they had gained access to fresh fruits and vegetables
that they otherwise would not have had. Some sample comments included:
Participants expressed that by participating in SFMNPP they experienced improved quality of life in terms of psychological as well as physical health. Several participants spoke of the home-delivered produce as being a surprise or a gift, and they indicated that the gift of fresh fruits and vegetables brought them joy. An 87-year-old female said, "I am extremely satisfied with the whole procedure. It's like getting a Christmas gift every other week. A nutritious one."
Theme 3: Newsletter-supported SFMNPP objectives
The newsletter was intended to support participant utilization of fresh
produce by providing nutrition education, food safety information, food
preparation hints and recipes, as well as information about SFMNPP and local
participating farmers. Almost all those interviewed indicated that they used
the newsletter to refer to the list of items in the bag. Only 3 of the 27
who were interviewed said that they did not regularly read the newsletter.
One person, who was legally blind, said that she could not read the
newsletter. Most of the participants said that they enjoyed reading the
newsletter and that it was useful and informative about the program and the
local farmers that grew the produce.
Theme 4: Participant satisfaction with SFMNPP
All of the subjects in this study stated that they wanted the program to
continue and they would sign up again if it were offered next year. When
asked for suggestions to improve the program, most of them said they liked
it the way it was. When pressed, they added suggestions about increasing or
adding items they liked, such as peaches, collard greens, potatoes, or
onions. A 73-year-old male said, "They've done all right by me. I don't
have any complaints about it. A little more would be nice, but I ain't gonna
be greedy." An 84-year-old female offered this: "I think it's very
good, if they want the elderly to stay in their homes."
Triangulation
Triangulation with other studies was carried out in 2 parts to validate data
and theme interpretation. First, we compared the findings of the SFMNPP
qualitative study with the results of the quantitative study (20). Second, we compared the
findings of the qualitative study with the ASE model (15).
The quantitative study results showed that participants in the SFMNPP increased their intake of fruits and vegetables during the 20 weeks of the program. The daily intake of fruits and vegetables increased 1.04 servings compared to a decrease of 0.27 servings for controls (95% CI, 0.68-1.95, P < .001). The overall positive attitude toward SFMNPP, the participants' utilization and enjoyment of the fresh produce baskets, and the measured outcomes of the increased number of servings of fruits and vegetables were consistent with the findings of the semi-structured interviews.
We applied SFMNPP findings to the ASE model (Figure 3). Issues mentioned by participants and identified by data analysis as relating to utilization of produce and satisfaction with SFMNPP fit into the scheme of the model shown. Reception to SFMNPP and belief in the health benefits of eating fruits and vegetables affected attitude. Delivery staff and SFMNPP newsletters affected social influence. Participants' belief in their ability to obtain and eat fruits and vegetables supported self-efficacy expectations. Encouragement, involvement of support systems, and increased knowledge about nutrition and local farming reduced barriers and promoted abilities. Thus, according to this model, barriers were minimized and abilities were reinforced to support intention to eat more fruits and vegetables.
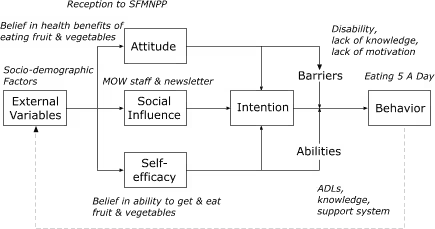
Figure 3.
Triangulation of Seattle Senior Farmers' Market Nutrition Pilot
Program Study Findings, 2001, with Attitude, Social Influence and
Self-Efficacy (ASE) Model. MOW = Meals on Wheels, ADL = Activities of
daily living. ASE model adapted from Brug et al (15). Reprinted with
permission from Elsevier.
Although we did not specifically ask study subjects about their health, they often volunteered personal health information that related to their motivation and ability to use the produce provided by SFMNPP. Thus, we identified health status and physical and cognitive disability as key factors influencing homebound seniors' intake of fruits and vegetables.
The participants' feedback regarding the program indicated their strong support for SFMNPP and the benefits that they felt they experienced because of the program. Seniors reported that they were healthier because they participated in the program. They said they were less constipated, felt better, and had better control of their diabetes. It would be difficult, if even possible, to measure joy and the program's positive effect on mental health, but these also were experiences that the participants related in the interviews. In the ASE model (Figure 1), the individual's attitude is important in determining the strength of his or her intention. In this model, strong intention can overcome barriers to the target behavior. While all of the interviewees said they ate most or all of the produce, probing revealed that the actual amount that they ate varied. Although disability appeared to be a significant factor preventing some seniors from fully utilizing the produce, physical disability was often overcome by those who were motivated. Thus, applying the findings to the model substantiated the importance of attitude. In the present study, many seniors made statements indicating they believed that eating fresh fruits and vegetables was good for their health. According to the model, having this belief or attitude would strengthen their intention to follow through with the target behavior and overcome potential barriers including physical disabilities.
The ASE model also helps to identify how participants overcame potential barriers to utilizing the fresh produce they received through SFMNPP. Participants with disabilities utilized more of the produce when they had assistance from an aide, a caretaker, family, or friends. Interactions with family and friends also could affect the seniors' motivation to overcome disabilities. Reading the newsletter or talking to the delivery person often overcame lack of knowledge about how to prepare items for eating. Finally, the behavior itself — eating more fruits and vegetables — reinforced the behavior by making seniors feel better.
It is likely that SFMNPP in Seattle and King County succeeded in increasing fruit and vegetable consumption among participants because it used a multi-pronged approach and addressed several components identified in the ASE model. While the homebound seniors were enjoying the fresh produce, they were also improving their health, reinforcing positive eating habits, strengthening their belief in the benefits of good nutrition, and extending their social network by getting help and sharing their SFMNPP experiences with others. By delivering the produce to homes, the program design eliminated 2 of the major barriers faced by many homebound seniors, namely their inability to go shopping and their lack of money to buy fresh fruits and vegetables. Thus, perceived self-efficacy increased with direct delivery of produce.
Another factor was the quality and variety of the produce. The homebound seniors who were interviewed were a diverse group representing different ages, races, ethnicities, social and economic backgrounds, and certainly different personalities and interests. While many considered themselves to be vegetable and especially fruit eaters, their taste preferences varied considerably. The freshness and variety of the produce was openly appreciated by a number of those interviewed. There was variety within each basket, the produce changed with the season, and participants received items they enjoyed. It was also stimulating for many of the seniors to receive more unusual items — mizuma, black pears, and fingerling potatoes — that they had never before eaten.
It is important to keep in mind some of the limitations of the present study and the use of qualitative methodology. Ideally, in a qualitative study the subjects would be individually selected to maximize representation of the diversity of the population under study. Our subjects volunteered to be interviewed. It is not known if and how these seniors differed from others who did not volunteer. For example, this study did not reveal themes regarding not wanting to continue with the program or general dissatisfaction with the program.
A limitation of the study design is inherent in the use of semi-structured interviews. The questions were both structured and open-ended in order to direct the focus of the interview and at the same time allow each subject to reveal issues that mattered to them. The semi-structured format with guided questions prevented the interviews from becoming too long, but it may have inhibited subjects from revealing themes that this study did not identify.
Our study identified several areas for future evaluations of Senior Farmers' Market programs.
Our qualitative study provides insight into why SFMNPP was successful in increasing fruit and vegetable intake among homebound seniors. Home delivery overcame the barriers of being homebound and having limited resources. In addition, the gift of locally grown fresh fruits and vegetables was a stimulating source of interest and encouragement to be healthy that was received by participants with anticipation and pleasure. The impact of this experience on the health of homebound seniors would be difficult to quantify but is nonetheless worthy of support.
This study was supported by Grant U48/CCU009654 from the Centers for Disease Control and Prevention to the University of Washington Health Promotion Research Center. We thank Sheryl Schwartz, Monica Jarrett and Adam Drewnowski for helpful discussions. We thank the seniors who participated in this study and our collaborators from Senior Services of King County, Pike Place Market Community Supported Agriculture, King County Area Agency on Aging, Public Health-Seattle & King County, and Washington State Aging and Adult Services Administration, Aging and Disability Services.
Corresponding Author: Donna B. Johnson, RD, PhD, Interdisciplinary Program in Nutritional Sciences & Center for Public Health Nutrition, Nutritional Sciences, University of Washington, Box 353410, Seattle, WA 98195. Phone 206-685-1068. E-mail: [email protected]
Author Affiliations: Lynne T. Smith, RD, PhD, MPH, Centers for Disease Control and Prevention, Community Guide Branch, Washington State Department of Health, Olympia, Wash. Work was done at Prevention Research Center and Nutritional Sciences Program, University of Washington, Seattle, Wash. Sharon Beaudoin, MPH, RD, CD, Healthy Mothers, Healthy Babies Coalition of Washington, Seattle, Wash; Elaine R. Monsen, RD, PhD, Interdisciplinary Program in Nutritional Sciences, University of Washington, Seattle, Wash; James P. LoGerfo, MD, MPH, Health Promotion Research Center, University of Washington, Seattle, WA.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
*Nonwhite subjects included 5 African Americans, 1 Native American, and 1 Puerto Rican.
|
|
|
|
|
|
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the authors’ affiliated institutions. Use of trade names is for identification only and does not imply endorsement by any of the groups named above.
Privacy Policy | Accessibility This page last reviewed March 30, 2012
|
|