 |
|
||||||||
|
|
| Home |
Volume 6: No. 3, July 2009
Suggested citation for this article: Hosey G, Aitaoto N, Satterfield D, Kelly J, Apaisam CJ, Belyeu-Camacho T, et al. The culture, community, and science of type 2 diabetes prevention in the US Associated Pacific Islands.
[Erratum appears in Prev Chronic Dis 2010;8(1). http://www.cdc.gov/pcd/issues/2011/jan/10_0212.htm.] Prev Chronic Dis 2009;6(3):A104.
http://www.cdc.gov/pcd/issues/2009/
jul/08_0129.htm.
PEER REVIEWED
Background
The type 2 diabetes epidemic is a global health issue, particularly in the US Associated Pacific Islands (USAPI). Population health approaches targeting policy development and environmental transformations can help prevent or delay diabetes and related complications.
Context
Since 1986, the Centers for Disease Control and Prevention, Division of Diabetes Translation has provided financial support to 6 USAPI jurisdictions for diabetes prevention and control programs. Geographic isolation, shortages of health care professionals, dependence on US and international aid, and persistent health care funding challenges are constant concerns in these jurisdictions.
Methods
In September 2007, representatives from USAPI diabetes prevention and control programs, the Papa Ola Lökahi
Pacific Diabetes Education Program, and the Division of Diabetes Translation met to collectively assess program goals within the Essential Public Health Services framework. Participants shared examples of integrated approaches to health promotion and diabetes
prevention.
Consequences
Despite persistent health care funding challenges, the assessment showed the resourcefulness of the islands’ diabetes programs in leveraging resources, creating policy and environmental interventions, and strengthening connections in the traditional cultural systems.
Interpretation
Population health approaches used in island jurisdictions reflect the resilience of the islands’ cultures in navigating between traditional and Western ways of life. Attention to the interface of cultural knowledge and Western science provides the USAPI diabetes prevention and control programs with opportunities to create strong, sustained partnerships with the shared vision of transforming social and environmental conditions so
that they can support healthy people
living in healthy island communities.
The type 2 diabetes epidemic, a global health issue, is severe in the US Associated Pacific Islands (USAPI) jurisdictions. Although a post-World War II US Navy survey of the Pacific islands found no cases of diabetes, subsequent population surveys have shown a dramatic increase in diabetes (1). In 2007, the estimated prevalence of diabetes for the US population (adults aged 20 years or older, diagnosed and undiagnosed) was 10.7% (2). Although USAPI diabetes surveillance data are limited, the 2001-2003 estimated prevalence for Guam was 11% (adults aged 18 years or older, diagnosed) (3); in 2002, the estimated prevalence for Pohnpei, an island state in the Federated States of Micronesia (FSM), was 32.1% (adults aged 25-64 years, fasting blood glucose [FBG] ≥126 mg/dL) (4) and for the Republic of the Marshall Islands (RMI) was 29.8% (adults aged 15-64 years, FBG ≥110 mg/dL) (5); in 2006, the estimated prevalence for the Republic of Palau was 38.9% (all ages, FBG ≥110 mg/dL) (6); and in 2004, the estimated prevalence for American Samoa was 47.3% (adults 25-64 years, FBG ≥110 mg/dL) (7).
In the USAPI, the proportion of people with diabetes who report self-care practices to prevent complications often falls below US levels. For instance, in Guam, 2001-2003 estimated prevalence of measured hemoglobin A1c (twice annually) was 56.7% and daily self-monitoring of blood glucose (SMBG) was 32.2%, significantly lower than US estimates for measuring hemoglobin A1c (65.9%) and daily SMBG (58.3%) (3). The rates of diabetes complications are also high. For example, in 2002 and 2003, the incidence of lower limb amputations secondary to diabetes for the RMI was 79.5 per 100,000 population (8), and lower limb amputations were performed on people as young as 30 years. When standardized to the 2001 European population, the amputation incidence rate in the RMI was approximately 400 per 100,000.
Population health approaches designed to improve diabetes outcomes in health care systems and to support and sustain healthy lifestyle choices can help prevent or delay diabetes and related complications (9,10). Improving population health depends on identifying and influencing the multiple health determinants (eg, socioeconomic position, physical environment, health care access) that can influence the health of a broad population (11). Population health interventions that use policy and environmental approaches can directly affect health behaviors or influence social norms (12). These potentially low-cost, high-reach approaches can lay the groundwork for future interventions, helping to reverse the increasing prevalence of diabetes and other chronic diseases (12).
In 1986, the Centers for Disease Control and Prevention (CDC), Division of Diabetes Translation (DDT) established partnerships with the USAPI to form diabetes prevention and control programs (DPCPs). The DPCPs use funding from CDC cooperative agreements to develop expertise in diabetes prevention and control, establish systems to define the prevalence of diabetes, identify gaps in diabetes care, evaluate limited intervention projects, and develop partnerships to leverage resources and extend outreach.
In the last few years, DDT professional staff reassignments interrupted the building of collaborative relationships with the USAPI DPCPs, promulgating uncertainty related to collective diabetes prevention goals. In an effort to realign the collaborative relationships and assess shared diabetes program goals, representatives from DDT and USAPI DPCPs met in September 2007. Using the Essential Public Health Services framework (13) as a conceptual foundation, we discuss the assessment process and describe several culturally specific, community-based diabetes prevention and control strategies established by the USAPI. We also explore the importance of acknowledging the interface between Western science-based practices and indigenous knowledge as an effective population health approach in indigenous populations.
Six USAPI jurisdictions have formal relationships with the United States: the US flag territories of American Samoa and Guam; the Commonwealth of the Northern Mariana Islands (CNMI); and the FSM (includes the islands of Chuuk, Kosrae, Pohnpei, and Yap); Republic of Palau; and the RMI, which are freely associated with the United States through compact agreements (1) (Figure 1). The population centers spread across 104 inhabited islands, covering an expanse of ocean larger than the continental United States. This geographic span, dependence on US and international aid, poorly maintained and equipped health care facilities, reliance on off-island tertiary and specialty care, and shortages of health care professionals create daunting health care challenges (1).

Figure 1. The US Associated Pacific Islands. Reproduced with permission from the Network Startup Resource Center, University of Oregon, Eugene, Oregon. http://www.nsrc.org/OCEANIA/oceania.html.
The prevalence of diabetes in the USAPI is increasing because of the islands’ rapid population and economic growth, coupled with ongoing transition from traditional ways of life (eg, communal farming and fishing) to Westernization (eg, more consumerism, with increased reliance on imported convenience foods, less physical activity) (1,14). Furthermore, a higher prevalence of obesity, 1 of the most common predisposing factors for type 2 diabetes (15), has followed on the heels of Westernization.
The USAPI annual per capita health care expenditure ranges from $140 in Chuuk to $1,032 in Guam; this stands in stark contrast to the annual US per capita expenditure of $5,711 (Table 1). Most islands depend on DDT funds to support their DPCPs. The average DDT funding award for the USAPI is $106,082, which covers administrative and staffing costs with modest support for community programs and outreach. Funding levels vary across jurisdictions depending on Congressional appropriations for the DDT competitive grant awards for DPCPs in the 50 states, territories, and island jurisdictions. Despite the persistent health care funding challenges amidst the growing epidemic of diabetes, the USAPI DPCPs have shown consistent capability and creativity in establishing partnerships across multiple sectors to leverage resources and broaden community outreach.
The USAPI is a culturally diverse region composed of traditional societies with a complex integrated web of social hierarchy and traditions related to values, spiritual beliefs, and relationships with the environment. Connectivity, reciprocity, and mutual assistance are customary within strong extended family and community networks (1,14). Additionally, the USAPI share a history of colonization, resulting in challenges to their sovereignty and subsequent loss of culture, land, voice, population, health, and well-being (14,16). However, even after years of foreign occupation and influence, the USAPI cultures remain vibrant (1). To understand the approaches necessary to protect the health of the people living in island communities, one must recognize the resilience of the Pacific peoples in upholding their cultural systems while navigating between indigenous and Western lifestyles, political and spiritual ideologies, and economic systems (14,16).
The Essential Public Health Services (EPHS) framework originated from the 1988 Institute of Medicine report, The Future of the Public’s Health in the 21st Century, which outlines 3 core public health functions: 1) assessment of health status, 2) assurance of quality and accessibility of health services, and 3) policy development (17). The core functions cover the key components of public health but were difficult to define and explain to the public, policy makers, and public health professionals. In 1994, representatives from government and national public health agencies established a broad consensus definition of the EPHS (17).
In 2003, recognizing the rapid change in the social, cultural, environmental, technological, and global environments that influence health, the Institute of Medicine released The Future of the Public’s Health in the 21st Century. This report suggested a broader scope for the EPHS and emphasized the need for an intersectoral public health system with links between government agencies and new partners (eg, communities, businesses, media) to transform the public’s health (17). The same year, DDT began supporting the EPHS as a framework for assessing DPCPs, specifically their capacity to expand intersectoral partnerships in an effort to strengthen diabetes public health systems (13). In this framework, a public health system creates benchmarks as it identifies its work in each service area. The EPHS can provide a roadmap for engaging partners in the environmental and societal transformations needed to prevent and control diabetes. Figure 2 shows a representation of the EPHS developed by the USAPI DPCPs.
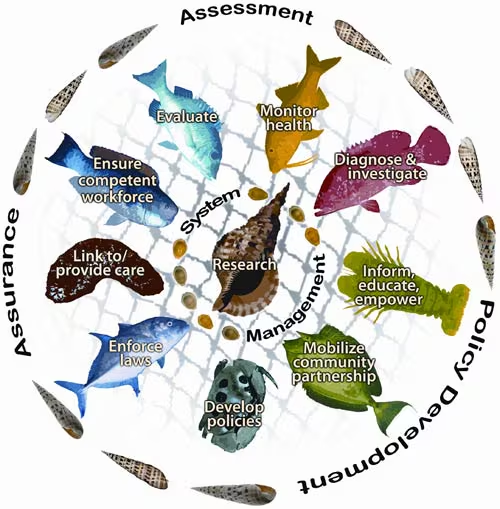
Figure 2. The Essential Public Health Services (EPHS) Pacific island graphic interpretation illustration. This is a representation of the EPHS developed by the US Associated Pacific Islands diabetes prevention and control programs. Overlaying the graphic is fish netting, a critical tool that helps to nourish and sustain island families and communities, symbolizing the integration and interconnectedness of each EPHS. Ocean life represents the essential services within the net and the 3 core public health functions surround the net. The central conch shell signifies research and system management, essential connectors among the EPHS.
Traditionally, USAPI DPCP meetings were held before large annual DDT meetings with state DPCP representatives. Breaking this pattern, DDT planned a 3-day participatory meeting in September 2007 with the 6 USAPI DPCP jurisdictions in Honolulu, Hawaii. A participatory approach is a colearning and empowering process that emphasizes the engagement of all partners as a method for research translation, systems and policy development, and community capacity building (18,19).
Because inclusion and democratic communication are key tenets of a participatory approach (18,19), we consulted with USAPI DPCP coordinators about meeting details such as date and location, possible agenda items, and suggested meeting facilitator(s). DDT and the USAPI DPCPs agreed to emphasize strengthening partnerships and co-learning during the meeting and to allow adequate time for USAPI DPCPs to share their strategies for building on local cultural strengths, knowledge, and resources to address health promotion and diabetes prevention needs. USAPI DPCPs collectively recommended the manager of the Papa Ola Lökahi Pacific Diabetes Education Program (PDEP), a champion of diabetes prevention with strong connectivity and understanding of the island cultures, as the meeting facilitator. Papa Ola Lökahi’s PDEP manager accepted the invitation to facilitate and helped plan the meeting.
To strengthen links with partners who worked in diabetes prevention in the Honolulu area, the meeting’s first day included the USAPI Primary Care Association, Pacific Island Health Officers Association, Micronesians United, and the Hawaii DPCP. Using the EPHS framework, the second and third days were reserved for equitable interchange and mutual understanding between DDT and USAPI jurisdictions about approaches to shared diabetes prevention goals. As the meeting progressed, an environment that fostered trust and relationship building developed, which allowed participants to unveil critical discussion topics, such as DDT staffing, future funding, and the urgent need for sustained diabetes and other chronic disease prevention efforts across island jurisdictions.
Several key outcomes with implications for future DDT and USAPI DPCP partnership practice emerged from this meeting. The open dialogue maintained throughout the meeting allowed DDT representatives to acknowledge the DPCPs’ contributions toward a shared CDC-USAPI vision of preventing diabetes and its complications among the people of the USAPI. The information shared affirmed the USAPI DPCPs’ commitment to community-based diabetes prevention focused on the strengths of each jurisdiction’s cultural system. DDT representatives also gained appreciation for the USAPI DPCPs’ skill in creatively leveraging scarce financial resources.
Using the EPHS framework, participants shared examples of integrated, intersectoral approaches in their jurisdictions. These approaches illustrated the creativity and resourcefulness of USAPI DPCPs in developing partnerships, applying policy and environmental interventions, and strengthening connections within the traditional cultural systems (Table 2).
These USAPI approaches also provide a link for supporting future DDT partnership practices that move beyond categorical single-sector diabetes programming to support efforts that build on strengths and assets of the USAPI partners and communities. The USAPI DPCPs cultivate partnerships with community, academic, and faith-based organizations, committed leadership (elected officials and traditional), and other public health system partners working toward sustainable community-based health promotion and disease prevention efforts. Examples of these approaches include
The meeting offered an opportunity for the DDT representatives, working with the meeting facilitator and USAPI DPCP participants, to realign collaborative relationships and common goals for continued USAPI capacity building. The stories shared during the meeting highlighted the success of using local cultural strength and knowledge to enhance opportunities for health promotion and diabetes prevention within USAPI communities. Recognizing the value of sharing these success stories with broader audiences that are also interested in addressing health disparities in their populations, the group presented an overview of island diabetes prevention efforts, called Casting Our Nets for Diabetes Prevention and Control — Pulling in Our Stories, at the DDT national conference, May 5-8, 2008, in Orlando, Florida. This was the first time the USAPI DPCPs have formally and collectively shared their stories about resourceful partnerships with CDC and other partners.
The USAPI DPCPs face challenges in building capacity for diabetes prevention not shared by mainland DPCPs. Nevertheless, the USAPI DPCPs have leveraged their community connections to enhance and support policy and environmental interventions. The connecting element among indigenous cultures is a strong traditional sense of unity with the environment (16). Approaches to health issues surrounding indigenous peoples need to consider their cultural knowledge and worldview. As the links between modern health problems and separation of people from their natural environment become clearer, the interface between cultural knowledge and Western-based science, coupled with participatory approaches, may help identify broad-ranging approaches to population health. Facilitating collaborative, equitable partnerships across the interface may also be a key element in empowering communities to effectively address the social and environmental determinants of health.
The USAPI DPCPs strive to create a balance between the diverse traditions that have shaped and sustained the USAPI with Western science’s evidence-based practices. This emphasis on balancing cultural knowledge and science provides the USAPI DPCPs opportunities to create strong, sustained partnerships with a shared vision: to transform social and environmental conditions to support healthy people living in healthy island communities. The Palau Ministry of Health added a service to its EPHS framework that addresses this vital concept: “Ensuring cultural integration in disease care, health protection, and health promotion” (21). The USAPI, with their development of innovative approaches to building capacity for diabetes prevention and control, may be in a unique position to contribute to the evolving knowledge and science base needed to reduce the prevalence of diabetes and other chronic diseases in populations around the world.
We are grateful for the involvement of several Pacific island representatives during this project, including Lynn Tenorio and Father Ryan Jimenez, Commonwealth of the Northern Mariana Islands; Kipier Lippwe, Federated States of Micronesia; Roselie Zabala and Frances N. Espres, Guam; Johannes Sermai and Donny Andrike, Republic of the Marshall Islands; and Megan Fong, Henry Ichiho, and JoAnn Tsark, Papa Ola Lökahi. We also thank Mr John Dax Moreno for sharing his artistic talent in the development of the US Associated Pacific Islands Essential Public Health Services graphic illustration.
Corresponding Author: Gwen Hosey, MS, ARNP, CDE, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Division of Diabetes Translation, 4770 Buford Hwy, Mailstop K-10, Atlanta, GA 30341. Telephone: 775-684-5907. E-mail: [email protected]. Ms Hosey is also a doctoral student at the Uniformed Services University of the Health Sciences, Bethesda, Maryland.
Author Affiliations: Nia Aitaoto, Papa Ola Lökahi, Pacific Diabetes Education Program, Honolulu, Hawaii; Dawn Satterfield, Jane Kelly, Centers for Disease Control and Prevention, Atlanta, Georgia; Carter J. Apaisam, DPCP Program Coordinator, Palikir, Pohnpei, Federated States of Micronesia; Tayna Belyeu-Camacho, DPCP Coordinator, Saipan, Commonwealth of the Northern Mariana Islands; Ione deBrum, DPCP Coordinator, Majuro, Republic of the Marshall Islands; Patrick Solidum Luces, DPCP Coordinator, Hagatna, Guam; Augusta Rengiil, DPCP Coordinator, Koror, Palau; Pasa Turituri, DPCP Coordinator, Pago Pago, American Samoa.
|
|
|
|
|
|
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Privacy Policy | Accessibility This page last reviewed March 30, 2012
|
|